




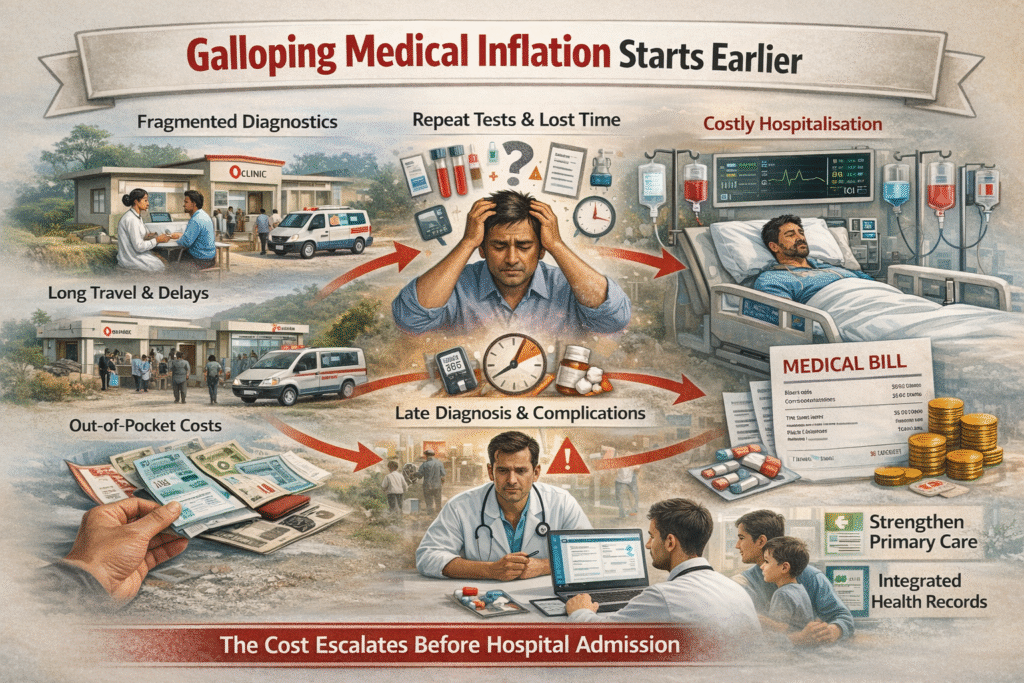
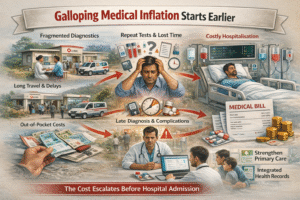
Hospital inflation in India is often discussed in the context of rising bed charges, surgical costs, or intensive care billing. Even before a patient is formally admitted, costs can start mounting due to fragmented diagnostics, delayed triage, and inefficiencies built into primary and secondary care processes.
Healthcare expenditure remains high at the household level despite policy efforts to expand insurance coverage. According to data from the Ministry of Health and Family Welfare and the National Health Accounts, out-of-pocket expenditure continues to account for a significant share of total health spending.
Patients often move between clinics, labs, and specialist centres before reaching a final diagnosis. Each step incurs direct and indirect costs, including repeat consultations, repeated testing, travel expenses, and lost income.
When conditions are identified at a later stage, treatment options are more intensive and correspondingly more expensive. This fragmentation can delay clinical clarity. When clinical records are not seamlessly shared across systems, tests are often repeated to confirm earlier findings. From an economic standpoint, duplication compounds cost inflation without necessarily improving quality of care.
In numerous instances, patients end up in hospitals not due to inherently complex conditions, but because early-stage care was inconsistent or delayed. In many Conditions such as hypertension and diabetes, they frequently go undiagnosed until complications emerge.
Clinical workflow structure also influences cost inflation. Primary healthcare systems are intended to function as the first line of detection and management. The patient has come for good and healthy improvement and is free from the disease. The clinical applications are very tough to manage. Taking care are must, and here the doctors are more liked by the people and give the first preference to the hospitals and this advance technologies in this generation.
In many regions, uneven infrastructure, limited resources, and capacity constraints can weaken this function. Secondary care facilities, in turn, must compensate by conducting fresh investigations or prolonged observation.
By the time a patient is admitted, the cumulative diagnostic process has already driven up costs. This inefficiency is not solely the result of individual decisions but is rooted in the design of the system, reimbursement structures, and unequal access to healthcare infrastructure.
Many insurance plans provide stronger reimbursement for hospitalisation than for early diagnostic intervention. This imbalance can unintentionally contribute to hospital cost inflation. When outpatient diagnostics and preventive monitoring are not adequately covered, patients may delay testing until symptoms worsen, increasing the likelihood of admission.
The way insurance products are structured influences both the timing and manner in which patients access hospital care. People in rural and semi-urban areas often have to travel long distances for tests or specialist appointments. Expenses for travel, lodging, lost wages, and other informal costs can create significant financial pressure even before hospitalisation. When early evaluation is unavailable or irregular, conditions may deteriorate by the time patients reach tertiary care facilities.
In this, the data is also fragmented and continues to fill the gaps also. The facilities are evolving nowadays very Fastly and it includes each and every one. Also, it contains financial pressure, which does not give you a free mind anytime. The semi-urban area is sometimes irregular and comes with certain conditions.
Continuity of health data is another key structural issue. When patient records are fragmented, healthcare providers do not have a complete picture of previous tests and outcomes. This uncertainty often results in precautionary admissions or repeated diagnostics, both of which drive up costs. Many symptoms are shown in many diseases. The healthy person and fit-minded person can work in a very easy manner. There are not an issue if you are living a healthy life and staying fit.
The conditions are improving day by day nowadays because people are more conscious about their health, and even people are teaching our young generations too. In today’s time, ai are creating so many things by itself so that the malfunctions reduce.
Treatable conditions become complex procedures. Routine monitoring gaps translate into emergency responses. The World Health Organisation has repeatedly emphasised that preventive care reduces long-term health expenditure.
In the Indian context, putting this principle into practice demands tackling fragmented diagnostics, inefficient referral processes, and misaligned reimbursement systems. Reducing inflationary pressure requires strengthening first-contact care, improving diagnostic continuity, and aligning incentives around early intervention.
Over the past decade, India’s healthcare expansion has considerably improved access. Moving forward, the focus will likely need to shift toward better integration of systems and coordination of clinical workflows. In this context, hospital cost inflation does not begin at the point of admission; it starts earlier, within the way care is accessed, managed, and escalated. Understanding this shifts the conversation from pricing alone to the broader design of the healthcare system.
Focus must shift to strengthening primary care, utilising digital health records, and improving diagnostics to reduce late-stage, high-cost hospitalisations. With medical inflation hovering around 13–14% annually, nearly double general inflation, the system must shift focus from pricing debates to care pathway redesign and early intervention models.
India’s next healthcare reform must address upstream inefficiencies, not just downstream hospital costs. It offers easy access to stories published on Money Control Pro and gives a little extra by setting out a context, an event or a trend that investors should keep track of.
Since the power sector sources most of its fuel, primarily coal, from within the country, it has been shielded from the recent price shocks and supply disruptions caused by the conflict involving Iran. In contrast, many of its Asia‑Pacific counterparts, like South Korea, Vietnam, Thailand and China, rely more heavily on imported fuels, leaving them more exposed to cost increases and pressure on earnings. Of course, this is not to say domestic companies have nothing to lose or gain from the current war in the Middle East. In fact, gas prices are rising and supply to industry is being cut. This can crimp production and lead to economic costs.
This can have a positive rub-off effect on local producers such as Coal India. While supplying a large portion of its output to power utilities, Coal India also sells certain quantities at market price linked to e-auctions. Higher international prices could boost auction rates and revenue for Coal India Limited. Unsurprisingly, its stock has risen by 4 per cent so far this week.
If more users turn to domestic coal, then the near-term existential risks feared for Coal India due to energy transition can be brushed aside for now. That said, the impact of the current market situation on Coal India’s sales volumes will be seen in the coming weeks and the next couple of months. Much depends on electricity demand.
Early forecasts also warn about the onset of El Nino weather conditions in 2026. It promises to be to be an interesting summer for Coal India.
More Stories
99% of heart attacks in India are linked to these 4 hidden risk factors know warning signs and proven prevention tipesheart attacks
‘Work shouldn’t consume every hour’: Indian tech professional on UK vs India office culture
Packaged food hurting productivity, mental health in young Indians: Report